


America's Right to National Bankruptcy and Healthcare
Politics / US Politics Jul 22, 2012 - 03:29 PM GMTBy: MISES

 Andrew Foy writes: People like me who believe the government should play a less active role in subsidizing healthcare costs are often asked the question "Do you believe healthcare is a basic human right?"
Andrew Foy writes: People like me who believe the government should play a less active role in subsidizing healthcare costs are often asked the question "Do you believe healthcare is a basic human right?"
While this is an important philosophical question to ponder, it often lends itself to unexamined answers and political demagoguery. The imprecise answer "yes" to this question by most governments around the world (including the United States) has served mainly to accelerate healthcare-cost growth and benefit the medical-industrial complex at the expense of the public. To appreciate this point, one must consider the reality of what having a right to healthcare, as it is presently understood, actually means, and then consider who wins.
 Does it mean that someone in a motor-vehicle accident has a right to emergency surgery that could save his life?
Does it mean that someone in a motor-vehicle accident has a right to emergency surgery that could save his life?
Does it mean that a teenager with leukemia has a right to potentially life-saving treatment?
Does it mean that a 60-year-old experiencing a major heart attack has a right to emergent therapy?
Does it mean that this same 60-year-old, after the heart attack is over, has a right to a cardiac rehabilitation program, routine office visits with a cardiologist, routine lab work, routine studies to monitor cardiac function, and life-long medications to control blood pressure, cholesterol, and diabetes knowing that doing these things will not eliminate the risk of another event but rather reduce it by a few percentage points a year?
Does it mean that this same person, 12 years down the road, has a right to an implantable cardioverter defibrillator, cardiac resynchronization therapy, and a left ventricular assist device for destination therapy when he eventually develops end-stage heart failure?
The above examples highlight the difference between health emergencies, which would qualify as insurable events, and other scenarios that fall under the category of health maintenance related to the progression of chronic illness, which would not be properly insurable under any rational insurance scheme. As it currently stands, all of the above cases are covered under most private insurance (now a requirement with the new healthcare law) and all public insurance plans. The right to healthcare has become synonymous with the right to medical insurance that covers all health related expenses — that's a big economic problem.
Friedrich Hayek wrote,
There is no objective standard for judging how much care and effort are required in a particular case; also, as medicine advances, it becomes more and more clear that there is no limit to the amount that might profitably be spent in order to do all that is objectively possible. Moreover, it is also not true that, in our individual valuation, all that might yet be done to secure health and life has an absolute priority over other needs. As in all other decisions in which we have to deal not with certainties but with probabilities and chances, we constantly take risks and decide on the basis of economic considerations whether a particular precaution is worthwhile, i.e., by balancing the risk against other needs.
Many who push the idea that healthcare is a right strive to eliminate all personal economic considerations that ultimately affect how an individual would balance health risks against other needs. They believe one should not have to balance such things. They strive to eliminate the distinction between health emergencies, which are insurable events, and health maintenance, which cannot be properly insured against. They incorrectly believe that all healthcare decisions are a matter of life and death. This is a tremendous boon to the medical-industrial complex.
Those who strive to eliminate the economization of healthcare decisions believe they are saving people. They are not. Regardless of their intentions, they are simply accelerating healthcare-cost growth. The equation that medical care equals health is mostly incorrect.
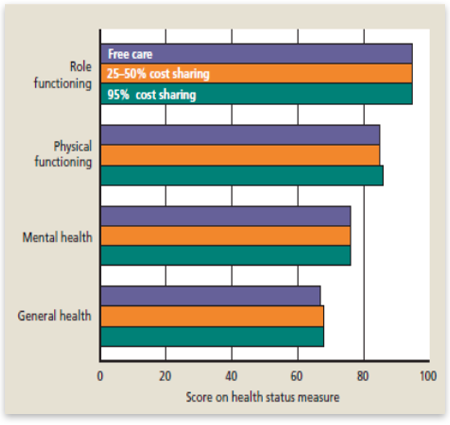
Medical care actually plays a limited role in determining our state of health. Many studies support this. The most important was the RAND Health Insurance Experiment, a large 15-year study that examined how different levels of cost sharing, ranging from none to 95 percent, affected both the use of medical care and health outcomes.[1] The results showed that cost sharing consistently reduced spending because patients actually sought less treatment. Those who had free care spent an average of 50 percent more per person per year than those with the highest level of cost sharing. However, despite differences in treatment, cost sharing had no adverse health effects. There were no significant differences between those with free care and those with cost sharing on any major health outcomes (figure 1).
What about the idea that as a society we should pay for health-maintenance services upstream to save on downstream healthcare costs? It sounds good but the data as presented above suggests the opposite — with few exceptions, paying for health maintenance upstream simply increases costs upstream without significantly impacting health downstream. This is true whether we are talking about primary or secondary prevention measures. In a previous article I wrote that
very few healthcare goods and services immediately impact whether an individual lives or dies and most of their benefits will go unnoticed. Instead, most of these goods and services, whether consumed in the inpatient or outpatient setting lower the medium or long-term risk of something or another by a few percentage points and in the end, we still die anyway. The value of this risk reduction is ultimately subjective.
This point cannot be emphasized enough.
Despite the above facts, benefit expansion continues unchecked, and this explains much of the extraordinary growth in healthcare costs over the last several decades (figure 2).
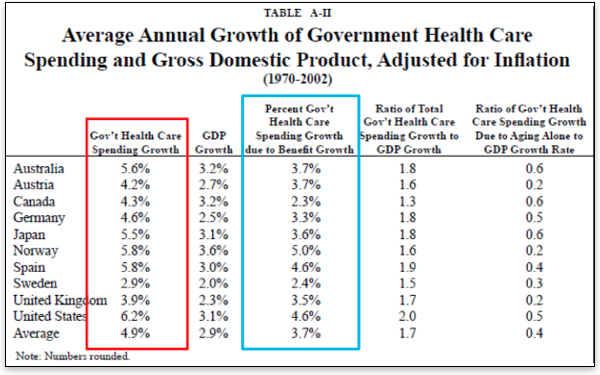
The data from Kotlikoff and Hagist clearly demonstrate that healthcare-cost growth is a worldwide problem.[4] And as the figure further demonstrates, the bulk of this cost growth is attributable to benefit expansion to cover an ever-increasing amount of goods and services related to health maintenance. The real winner of this benefit expansion is the medical-industrial complex.
The cost growth we see in healthcare is clearly not the result of unfettered free markets. While many make the spurious claim that the United States enjoys a free-market healthcare system, they do not argue this for most of the other countries included in Kotlikoff's analysis.[5]
Therefore, the argument that extraordinary healthcare-cost growth in the United States results from the free market is easily disproven. Rather, it results from benefit expansion that is either directly subsidized by or regulated by the government just as in the other countries studied.
In fact, one of the main reasons America enjoys the highest healthcare costs per capita and the most excessive healthcare-cost growth is because we have the most generous healthcare entitlement in the world: Medicare.
Kotlikoff and Hagist analyzed the ratio of healthcare spending based on age group and found that for individuals 65 and older the United States significantly exceeds all the other countries (figure 3).
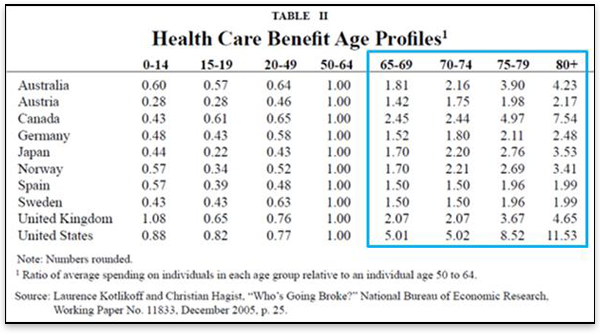
As figure 3 demonstrates, Medicare is the most profligate entitlement program in the world. In a review of the literature, Levy and Meltzer identified three high-quality studies examining the Medicare population and the effect Medicare had on health outcomes. They found that "Medicare increases consumption of medical care and may modestly improve self-reported health but has no effect on mortality."[7] Finkelstein and McKnight used data from the 1960s to see whether geographic areas with lower insurance coverage rates prior to the enactment of Medicare experienced improvements in mortality following the enactment of Medicare relative to areas with higher pre-1965 coverage rates. They found that while hospital utilization and spending increased significantly, "In its first 10 years, the establishment of universal health insurance for the elderly had no discernible impact on their mortality."[8] These findings are consistent with those of the RAND health-insurance experiment and reinforce the notion that medical care plays a relatively limited role in one's overall health.
It should be clear from what has been outlined above that benefit expansion to include an ever-increasing and complex array of mostly nonemergent medical goods and services is responsible for the extraordinary healthcare-cost growth we see in the United States and around the world.
Now I would like to return to the question of rights. What exactly does the right to healthcare entail: only services that provide an immediate and tangible life-saving benefit? Should it also include those that have a significant and tangible impact on the quality of one's life? How about those services that can decrease one's risk of dying by 50 percent a year or 25 percent or 5 percent or 0.5 percent? What about services that cost $35,000 per quality-adjusted life year saved — or how about $250,000? Why not just anything even tangentially associated with one's health like having a higher salary, living in a bigger house, or driving a nicer car? As far as that goes, let us be reminded by Hayek, there is no limit. As a physician, I can attest to that.
To be clear, I do not believe healthcare is a right. I believe in the nonaggression principle and thus the provision of medical goods and services at the involuntary expense of someone else (and yes, taxes are involuntary unless you personally volunteer to pay them) is actually a rights violation. But I can accept a basic level of healthcare coverage as a condition or provision of democratic citizenship; however, it should be limited to true health emergencies. And even in the case of emergencies, therapies must be limited by some objective and well-defined formula such as cost per quality-adjusted life years saved cannot exceed X. Anything outside this scope should have to be paid for through personal savings or provided by charity. This must be the case if there is any chance to make such a provision economically feasible over the long run. It would also preserve the market function for the vast majority of medical goods and services making them more affordable and accessible for everyone.
In closing, I want to briefly discuss the recently upheld Patient Protection and Affordable Care Act (PPACA) and its implications for healthcare-cost growth in the United States. Its proponents professed two main intentions: (1) to insure the uninsured, and (2) to bend the healthcare cost curve down. While it will achieve the first objective, it will certainly exacerbate the problem of healthcare-cost growth — achieving the exact opposite of its stated intentions.
Keehan and colleagues, from the Actuary Office of the Center for Medicare and Medicaid Services (CMS), recently published national healthcare spending projections through 2020. According to the authors,
In 2014, national health spending growth is expected to reach 8.3 percent when major coverage expansions from the Affordable Care Act of 2010 begin. The expanded Medicaid and private insurance coverage are expected to increase demand for health care significantly, particularly for prescription drugs and physician and clinical services.[9]
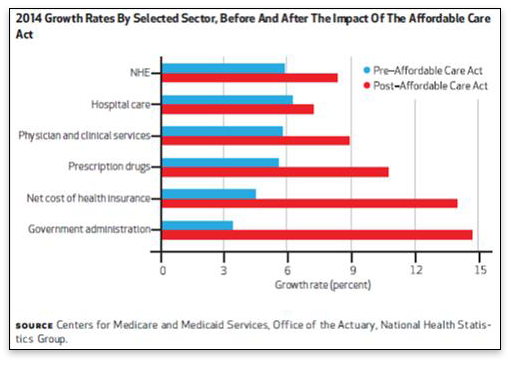
The findings from the Actuary Office enforce the ideas presented throughout this paper — that subsidizing medical care in the PPACA will significantly increase consumption and thus cost growth. This will come almost entirely from nonemergent services and administration costs, as figure 4 demonstrates. Even the "hospital-care" cost growth included in the figure will come from nonemergent hospitalizations for things such as "same-day" procedures, which are not life saving.
Overall, the PPACA will not affect health outcomes, but it will increase healthcare costs for everyone. The only thing clear about the right to healthcare is that it is synonymous with the right to national bankruptcy.
Andrew Foy is cardiology fellow at Penn State-Hershey University Medical Center. The opinions expressed here are his own and are not intended to represent those of his employer. Send him mail. See Andrew Foy, MD's article archives.![]()
You can subscribe to future articles by Andrew Foy, MD via this RSS feed.
© 2012 Copyright Andrew Foy - All Rights Reserved Disclaimer: The above is a matter of opinion provided for general information purposes only and is not intended as investment advice. Information and analysis above are derived from sources and utilising methods believed to be reliable, but we cannot accept responsibility for any losses you may incur as a result of this analysis. Individuals should consult with their personal financial advisors.
© 2005-2022 http://www.MarketOracle.co.uk - The Market Oracle is a FREE Daily Financial Markets Analysis & Forecasting online publication.